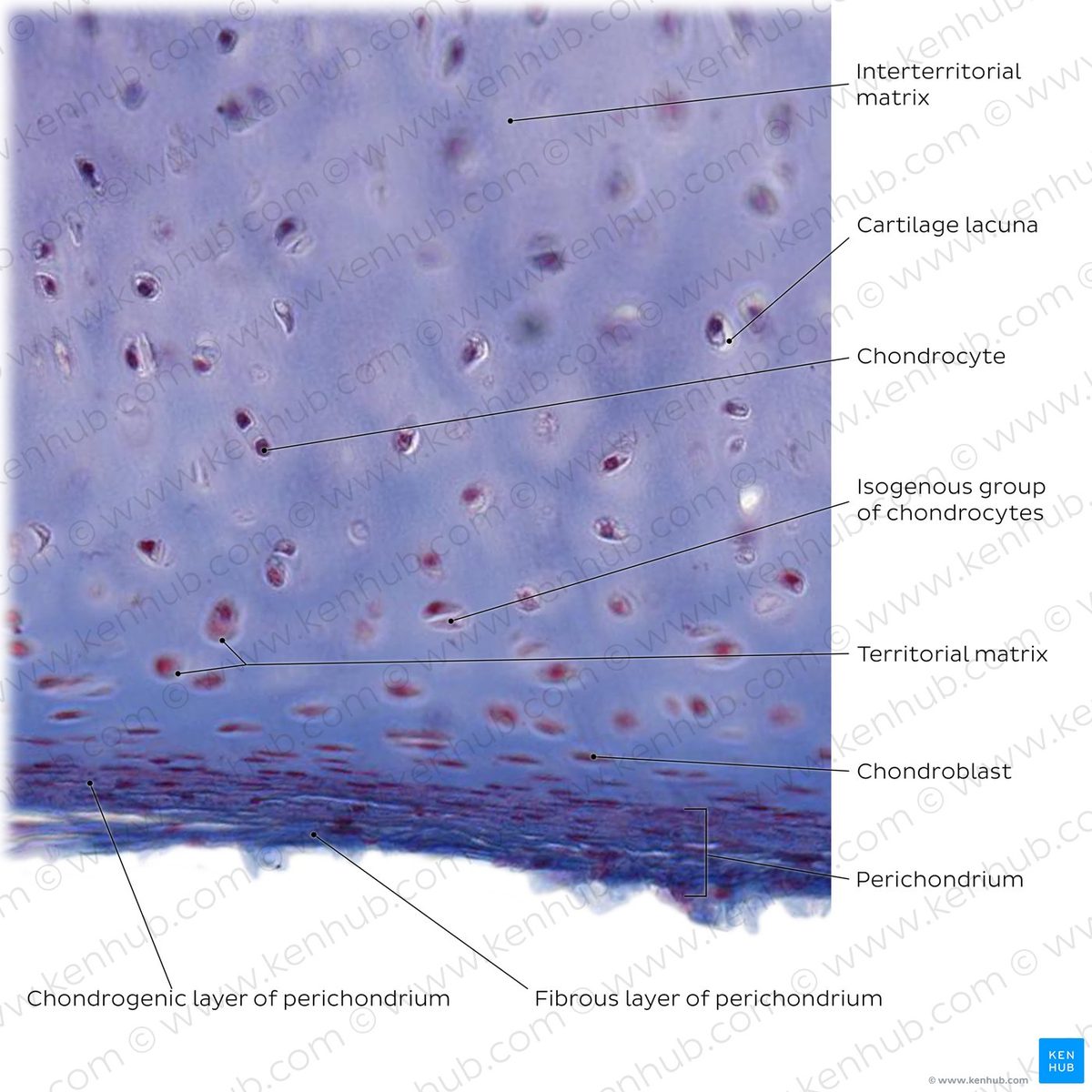
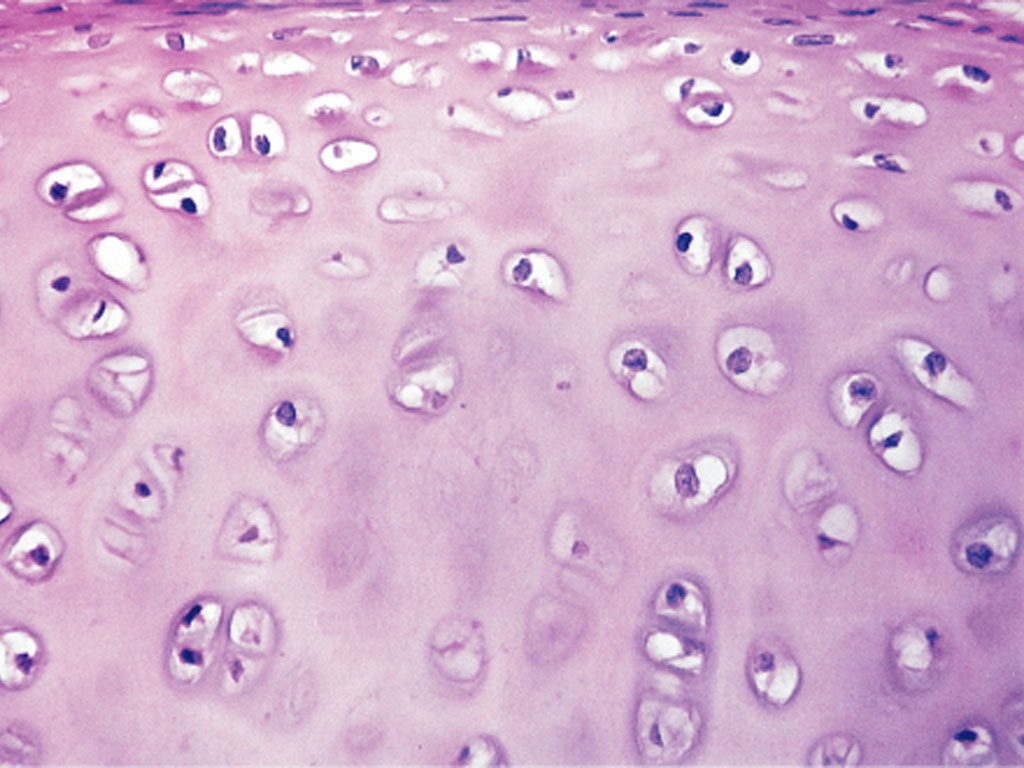
A November 2025 study in Science showed that blocking an enzyme called 15-PGDH regrew cartilage in older mice and in human joint tissue from knee replacement patients. Blocking it shifts cartilage cells from degrading to rebuilding—without stem cells.
Epirium Bio, which holds the exclusive license to Stanford's 15-PGDH patents, completed Phase 1 with 88 participants and no dose-limiting toxicities. Phase 2b enrollment for sarcopenia is planned for H2 2026. A Fast Track Designation application was due to the FDA in Q2 2026.
Why it matters
No drug has ever reversed cartilage loss; if this works, 700,000 knee replacements a year become avoidable.
16 events
Latest: May 2nd, 2026 · 2 months ago
Showing 8 of 16
JK to step
Tap a bar to jump to that date
Jump to
May 2026
15-PGDH Inhibitors Show Efficacy in Gut Inflammation Models
LatestConference Presentation
At Digestive Disease Week in Chicago, Epirium presented preclinical data showing MF-300 and a second compound, MF-1305, improved outcomes in mouse colitis models. MF-300 matched anti-IL-12/23 biologic response rates at all doses, suggesting 15-PGDH inhibition may apply to inflammatory bowel disease as well as muscle and cartilage.
April 2026
Renovare Therapeutics Launches with ARPA-H Funding for Competing Osteoarthritis Approach
Industry
CU Boulder's ARPA-H NITRO team advances to the next phase of up to $33.5 million in federal funding. Spinout Renovare Therapeutics launches to commercialize slow-release intra-articular injections and biomaterial repair kits for osteoarthritis. Human trials are targeted for 2028.
March 2026
Epirium Bio Presents MF-300 Phase 1 Data at ICFSR 2026
Conference Presentation
At the Intrinsic Capacity, Frailty and Sarcopenia Research Conference in Washington, DC, Epirium presented Phase 1 data from 88 participants. No dose-limiting toxicities were observed at any dose, including in adults aged 65-75. Phase 2b enrollment remains on track for H2 2026.
February 2026
Popular Mechanics Features Stanford Cartilage Breakthrough
Media Coverage
Major science publication highlights Stanford's cartilage regeneration findings and clinical translation pathway. Reports that researchers hope to run Phase 2 trials for cartilage regeneration following successful muscle trials.
January 2026
FDA Type C End-of-Phase 1 Meeting Yields Positive Outcome
Regulatory
Epirium Bio announces successful Type C meeting with FDA. Alignment gained on Phase 2b inclusion/exclusion criteria, primary and secondary endpoints, trial design, sample size, and dosing regimen. Company plans to file Fast Track Designation application in Q2 2026.
Stanford Breakthrough Gains Widespread Attention
Media Coverage
News coverage highlights potential for the treatment to make joint replacements obsolete, spurring discussion of clinical timeline.
Positive Results in Older Adults Announced
Clinical Trial
Epirium reports MF-300 is well tolerated in adults over 65, with pharmacodynamic profile consistent with younger participants.
November 2025
Science Publishes Cartilage Regeneration Results
Publication
Stanford team publishes study showing 15-PGDH inhibitor regrows cartilage in aged mice and human tissue samples from knee replacement patients.
September 2025
Phase 1 Shows Safety and Target Engagement
Clinical Trial
Epirium announces MF-300 is well tolerated with no discontinuations. Biomarkers confirm the drug hits its target.
January 2025
First Humans Dosed with 15-PGDH Inhibitor
Clinical Trial
Epirium Bio begins Phase 1 trial of MF-300, the first 15-PGDH inhibitor tested in humans, targeting sarcopenia.
January 2023
Gerozyme Term Coined
Research Milestone
Blau lab formally defines 'gerozyme' class of enzymes that increase with age and drive tissue function loss across multiple organ systems.
December 2022
First Cartilage Implant Gets FDA Premarket Approval
Regulatory
Agili-C, a biodegradable implant for cartilage and bone regeneration, becomes first to receive FDA Premarket Approval after Breakthrough Device designation.
January 2021
Blau Lab Identifies 15-PGDH as Aging Regulator
Research Milestone
Stanford researchers discover that the enzyme 15-PGDH accumulates in aging muscles and drives tissue decline.
December 2016
FDA Approves MACI
Regulatory
FDA approves MACI, an autologous cell therapy for cartilage defects. Earlier product Carticel is phased out the following year.
January 1994
First Cell Therapy for Cartilage in Humans
Research Milestone
Autologous chondrocyte implantation (ACI) is first performed in humans, marking the beginning of cell-based cartilage repair approaches.
January 1743
Hunter Declares Cartilage Cannot Heal
Historical
Surgeon William Hunter writes that damaged cartilage 'is never recovered'—a statement that defined medical understanding for centuries.
Historical Context
3 moments from history that rhyme with this story — and how they unfolded.
1 of 3
1987-Present
Autologous Chondrocyte Implantation (1994)
Swedish surgeon Lars Peterson performed the first human autologous chondrocyte implantation in 1994, after proving the concept in rabbits in 1987. The procedure harvests a patient's own cartilage cells, grows them in a lab, and reimplants them into the joint. Carticel became the first FDA-approved cell therapy for cartilage in 1997.
Then
ACI established that cartilage regeneration was possible, spawning a new field of cell-based therapies and multiple commercial products.
Now
Despite 30 years of development, ACI and its successors remain limited to focal defects in younger patients. They cannot treat the diffuse cartilage loss of osteoarthritis and require surgery. No cell therapy has become standard of care for age-related cartilage degeneration.
Why this matters now
The Stanford approach bypasses the core limitation of cell therapies: it doesn't require transplanting cells. Instead, it reactivates the patient's existing chondrocytes, potentially enabling treatment of the diffuse damage characteristic of aging.
2 of 3
1990s-Present
Disease-Modifying Osteoarthritis Drug Failures
Pharmaceutical companies have spent billions pursuing DMOADs—drugs that could slow or reverse cartilage loss rather than just manage pain. Candidates targeting matrix metalloproteinases, nerve growth factor, Wnt signaling, and other pathways have failed in clinical trials. As of 2025, neither the FDA nor European regulators have approved any DMOAD.
Then
Each failure refined understanding of osteoarthritis complexity but left patients with only symptom management options.
Now
The regulatory pathway for DMOADs remains undefined, with debates over appropriate endpoints (pain reduction vs. structural improvement vs. function). Companies have grown cautious about osteoarthritis drug development.
Why this matters now
The Stanford 15-PGDH inhibitor faces the same regulatory uncertainty but approaches the problem differently—targeting an aging mechanism rather than a specific disease pathway. Its success in muscle trials may help establish the regulatory path.
3 of 3
2008-2025
Prostaglandin E2 Research Paradigm Shift
For decades, elevated PGE2 in arthritic joints was viewed as harmful, leading to widespread use of NSAIDs and COX-2 inhibitors to suppress it. Research beginning around 2008 revealed a paradox: at low concentrations, PGE2 is actually chondroprotective. The key wasn't how much PGE2 was present, but how quickly it was being degraded by 15-PGDH.
Then
This complicated the simple 'inflammation is bad' model that had guided drug development.
Now
The insight that preserving PGE2 rather than suppressing it could be therapeutic opened an entirely new drug development strategy.
Why this matters now
The Stanford approach directly applies this paradigm shift: rather than suppressing inflammation, it preserves the beneficial effects of PGE2 by blocking the enzyme that degrades it.