Smallpox Eradication Campaign (1967-1980)
WHO launched an intensified campaign to eliminate smallpox, a disease killing 300 million people in the 20th century alone. The $300 million effort combined mass vaccination with targeted surveillance-containment strategies. The US and Soviet Union cooperated despite Cold War tensions. The last natural case occurred in Somalia in 1977.
WHO certified global eradication in December 1979, making smallpox the first human disease eliminated.
The campaign saves over $1 billion annually in vaccination costs alone. It established the model for coordinated global health campaigns and proved disease eradication was achievable.
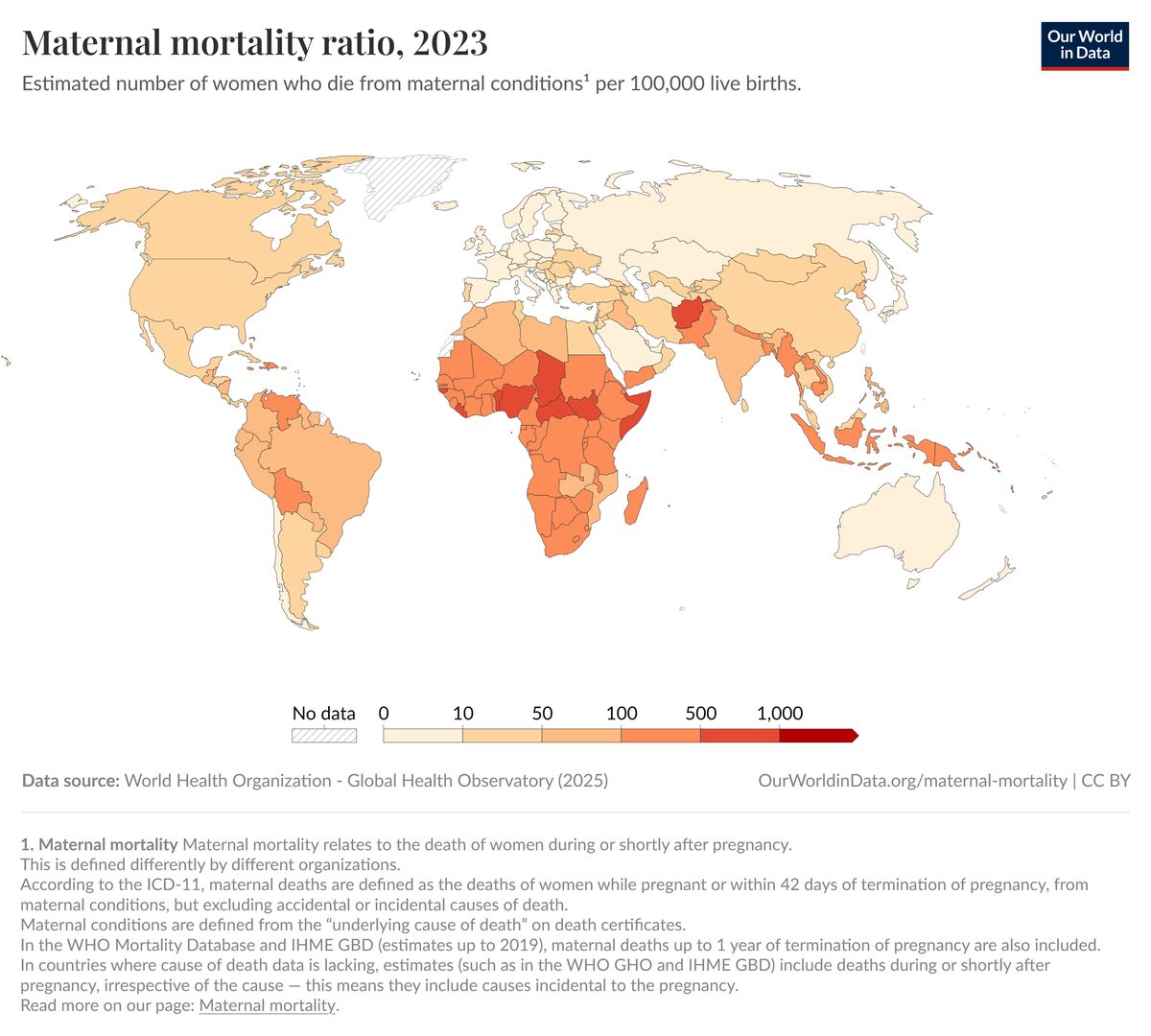
Like maternal mortality reduction, smallpox eradication required sustained international coordination, standardized interventions, and investment in health infrastructure in low-income countries. Both campaigns faced skepticism about feasibility and required decades of effort.