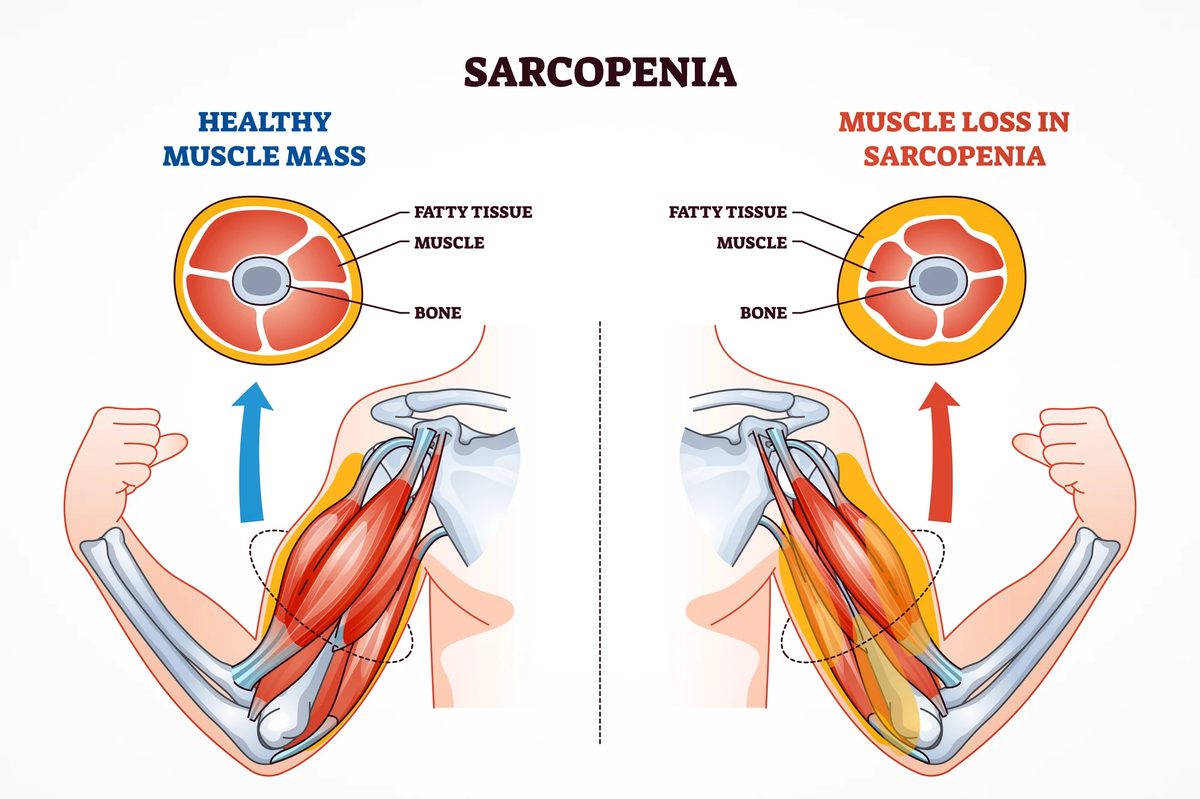
The biggest knock against blockbuster weight-loss drugs like semaglutide is that up to 40% of weight lost is lean tissue (muscle and bone), not fat. New therapies entering trials target genes to spare muscle.
On March 26, 2026, Wave Life Sciences tested RNA-silencing drug WVE-007. A single injection cut visceral fat by 14.3% over six months while patients gained 2.4% lean mass — a profile no other obesity drug matches. This exemplifies one of several emerging approaches that could reshape a market Goldman Sachs projects will reach $95–130 billion by 2030.
Arrowhead targets the same liver gene with RNA therapy, and combining it with tirzepatide doubles weight loss. Rivus Pharmaceuticals is testing an oral pill that accelerates metabolism in fat cells specifically. If any of these mechanisms prove safe and effective at scale, they could complement or compete with GLP-1 drugs — redefining what 'weight loss' means in clinical practice from simply pounds lost to tissue quality.